
Minimum effective dose training is defined as the smallest exercise stimulus needed to produce meaningful strength or muscle adaptation. Not the least effort you can get away with. The smallest effective stimulus. That distinction matters enormously if you are over 40 and trying to get stronger without wrecking your schedule or your joints. What is minimum effective dose training, really? It is a framework borrowed from pharmacology and applied to resistance training. Get the dose right and you adapt. Go below it and nothing happens. Go too far above it and recovery becomes the problem.
What does the science say about minimum effective dose training?
The research on this is clearer than most fitness content lets on. The ACSM's 2026 position stand confirms that meaningful strength gains require lifting at or above 80% of your one rep max, across 2–3 sets per exercise, at least twice per week. That is the floor. Variables like training to failure, rest interval length, and set structure did not consistently change outcomes once those core variables were met. That finding alone should simplify how you think about program design.
"Minimum effective dose is not minimum time spent regardless of effort. It is minimum effective stimulus." — IDEA Health & Fitness Association
The IDEA Health & Fitness Association makes this point directly. Lower volume can maintain and even build strength, but only when intensity stays high. Drop the weight and the sets together and you have crossed below the threshold. Nothing adapts.
A 12-week randomized trial in older women tested minimal dose resistance training using roughly two sessions per week with single sets. Strength improved. But the proportion of high responders was low, and outcomes were not consistently superior to higher-volume approaches. The takeaway is not that MED fails. It is that MED is individual. Some people respond well to the floor dose. Others need more volume to cross their personal adaptation threshold.
There is also a cognitive angle worth knowing. A 12-week resistance training trial in older women found that both 8–12 RM and 10–15 RM intensity ranges improved cognitive function, with MoCA scores rising by 2.9%–5.2% and depression scores dropping significantly. You are not just training your body when you lift. That matters for anyone over 40 thinking about long-term health, not just aesthetics.
Key evidence points:
- Strength gains require loads at or above 80% of 1RM, 2–3 sets, at least 2 sessions per week
- Hypertrophy requires higher weekly volume, at least 10 sets per muscle group per week
- Single-set, low-frequency protocols improve strength but show high individual variability in older adults
- Cognitive and mental health benefits appear across a broad range of training intensities
How does MED differ for strength versus hypertrophy goals?
The minimum training threshold is not a single number. It shifts depending on what you are trying to accomplish. This is where most people get confused, and where a 2026 systematic review in Sports Medicine confirms the difference. Strength and hypertrophy respond to different dose variables. Treating them the same leads to programs that are either too light to build muscle or too heavy and fatiguing to sustain.
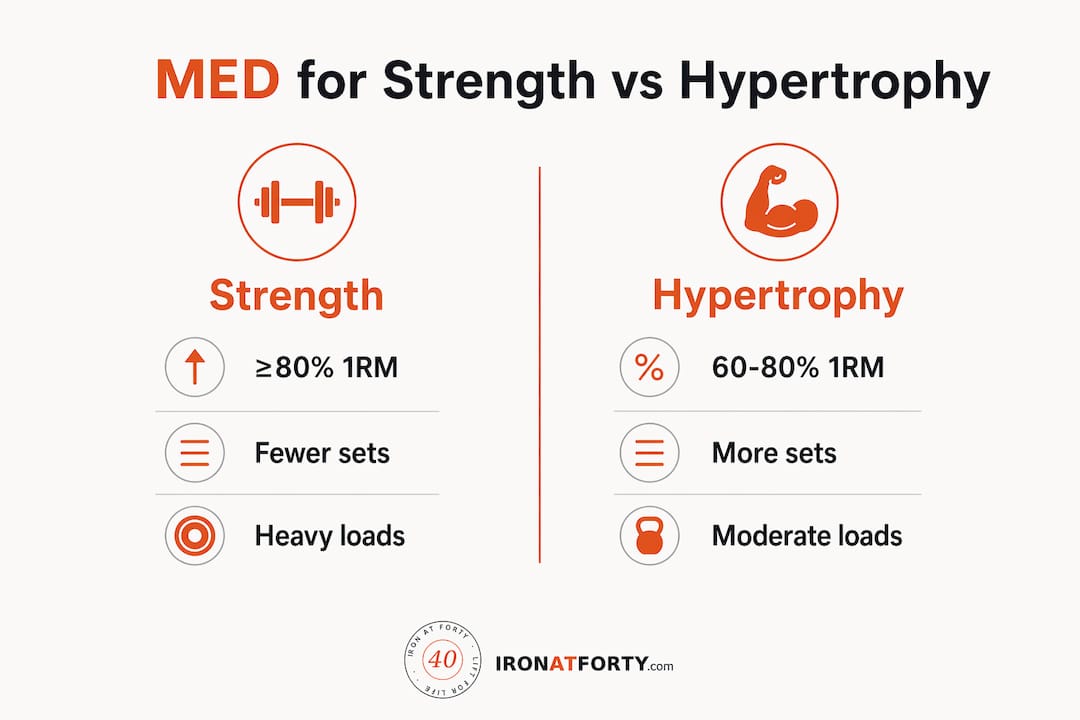
| Variable | Strength MED | Hypertrophy MED |
|---|---|---|
| Load | ≥80% 1RM | 60–80% 1RM |
| Weekly sets per muscle | 2–3 sets per session | ≥10 sets per week |
| Sessions per week | 2+ | 2–3 |
| Proximity to failure | Not required | Closer to failure helps |
| Primary focus | Intensity | Volume |
Strength responds best to heavy loads with lower total volume. Hypertrophy needs more total weekly sets, even at moderate loads. If your goal is to stay strong and functional after 40, the strength MED is actually more manageable. Two sessions per week, three sets of compound lifts at a challenging weight. That is a realistic floor.
Effort quality matters as much as volume. Reps in reserve (RIR) is a practical way to gauge this. Finishing a set with 2–3 reps left in the tank is enough to drive adaptation without grinding into failure every session. Failure training is not required for results, and for adults over 40, it adds recovery cost without proportional benefit.
Pro Tip: Track your reps in reserve on your two hardest sets each session. If you consistently finish with 4 or more reps left, the weight is too light to count as an effective stimulus.
What practical strategies work best for adults over 40?
Applying minimum effective dose fitness principles to a real program comes down to four decisions: exercise selection, load, frequency, and progression. Get those right and the rest is detail.
Peter Attia's 2026 protocol offers one of the clearest practical frameworks. Two sessions per week. Moderate loads in the 8–12 rep range. Three to four sets per exercise. No training to failure. Compound movements only. The goal is adherence and consistent stimulus, not chasing the theoretical minimum. Attia's framing is useful because it acknowledges that the barrier to starting is often psychological, not physiological.
Here is how to structure a practical MED program for adults over 40:
- Choose compound movements. Squats, deadlifts, rows, presses, and carries cover most of what you need. Single-joint isolation work is optional at this stage.
- Train twice per week minimum. Two sessions per week hits the training frequency threshold for strength adaptation. Three sessions per week is better for hypertrophy.
- Use loads at or above 80% of your working max. For most people, this means the last two reps of each set feel genuinely hard. Not impossible. Hard.
- Do 2–3 sets per exercise. More is not always better. Quality of each set matters more than total set count at the MED level.
- Progress every 2–3 weeks. Add weight or reps when you can finish your sets with only 1–2 reps in reserve. Stagnation means you have drifted below your effective dose.
- Reassess every 12 weeks. Physiological and cognitive gains from resistance training respond to adjustment cycles roughly every 12 weeks. Use that window to evaluate whether your current dose is still working.
Pro Tip: If you only have 30 minutes, do not cut the weight. Cut a set. Intensity is the non-negotiable variable. Volume is the lever you adjust.
Consistency beats intensity at the MED level. A program you run for 12 months at 80% effort beats a perfect program you abandon after six weeks. Training consistency after 40 is the real multiplier. The dose only works if you keep showing up.
How do you track and adjust your personal minimum effective dose?
What is optimal training intensity for you specifically? That question has no fixed answer. Your MED is dynamic. It shifts as you get stronger, as life stress changes, and as your recovery capacity fluctuates. The concept of dose response applies here directly. What is dose response in this context? It means your body adapts to a given stimulus, and once adapted, that same stimulus no longer drives further change. You need to adjust the dose upward to keep progressing.
Practical tracking methods that work for adults over 40:
- Strength PRs on key lifts. If your squat, press, or deadlift numbers are not moving over a 4-week period, your dose is likely too low or your recovery is compromised.
- Mood and energy levels. Consistent fatigue, poor sleep, or irritability after training sessions signals you have gone above your recovery capacity, not below your MED.
- Workout completion rate. If you are skipping sessions or cutting sets short regularly, the program is too demanding. Scale back to a dose you can actually sustain.
- Cognitive feedback. Given the mental health benefits shown in resistance training research, tracking mood and mental sharpness is a legitimate adaptation marker, not just a soft metric.
Dropping volume too low is a real risk. Research on minimal dose resistance training in older adults shows that a low proportion of people respond well to the absolute floor dose. If you stall, the answer is usually a modest increase in weekly sets, not a complete program overhaul. Add one set per session and reassess over four weeks. Use a training progress tracker to make that evaluation objective rather than guesswork.
Weekly volume distribution also matters. Hitting 10–12 sets per muscle group per week across two sessions is more effective than cramming all of it into one long session. Spreading the weekly training volume reduces per-session fatigue and keeps technique sharp. That is especially relevant after 40, when recovery between sessions takes longer.
Key Takeaways
Minimum effective dose training works because it targets the precise stimulus threshold for adaptation, not the maximum volume your schedule can absorb.
| Point | Details |
|---|---|
| MED is stimulus-based, not time-based | Lower volume only works when intensity stays at or above 80% of your working max. |
| Strength and hypertrophy have different floors | Strength needs heavy loads and 2+ sessions per week; hypertrophy needs at least 10 sets per muscle weekly. |
| MED is individual and dynamic | Research shows high variability in older adults; reassess your dose every 12 weeks. |
| Consistency is the real multiplier | A manageable program done for 12 months beats a perfect program abandoned in six weeks. |
| Cognitive benefits are real | Resistance training at moderate loads improves cognitive function and mood in adults over 40. |
The uncomfortable truth about "doing less"
I have worked with enough people over 40 to know how MED gets misapplied. Someone reads that two sessions per week is enough, so they start lifting light weights for a few sets and wonder why nothing changes after three months. That is not minimum effective dose training. That is just low-effort training dressed up in scientific language.
The word "minimum" is the trap. People hear it and think easy. What it actually means is the minimum stimulus that forces your body to adapt. That stimulus has to be uncomfortable. The sets have to be genuinely hard. The load has to be high enough to matter. If you finish every set feeling like you could have done ten more reps, you are below the threshold. Nothing is happening.
What I find works best for people over 40 is treating MED as a floor, not a ceiling. Two sessions per week is the floor. Eighty percent of your one rep max is the floor. Two sets per exercise is the floor. Build from there based on how you respond. Some people thrive on three sessions and four sets. Others genuinely do well at the minimum. You will not know until you test it honestly, with real intensity, for at least 12 weeks.
The other thing worth saying: MED aligns beautifully with life after 40. You have work, family, and a body that needs more recovery time than it did at 25. A program built around the effective minimum is not a compromise. It is a realistic, sustainable approach to staying strong for decades. That is worth more than any six-week blast program.
— Jeff
Ironatforty tools built for serious training after 40
Ironatforty exists for lifters who want real guidance without the gym bro noise. Every article, tool, and guide is built around the reality of training after 40, not recycled advice written for 22-year-olds.
If you are applying minimum effective dose principles to your program, the free training and nutrition tools at Ironatforty give you a practical starting point. Use the TDEE calculator to align your calorie intake with your actual training output. A two-session-per-week MED program burns fewer calories than a five-day split. Your nutrition needs to reflect that. Head to Ironatforty for science-backed training guides written specifically for adults who lift and want to keep lifting for the long haul.
FAQ
What is minimum effective dose training?
Minimum effective dose training is the smallest exercise stimulus needed to produce meaningful strength or muscle adaptation. It is defined by intensity and frequency, not just session length.
How many days per week do I need to train for MED results?
The ACSM confirms that two sessions per week at loads at or above 80% of your one rep max is the minimum threshold for strength gains. Hypertrophy requires higher weekly volume, typically across two to three sessions.
Is minimum effective dose training safe for adults over 40?
Yes. Research in older adults shows strength and cognitive benefits from two-session-per-week protocols at moderate to heavy loads. The key is maintaining intensity while managing recovery between sessions.
Can I build muscle on a minimum effective dose program?
You can build muscle, but hypertrophy requires at least 10 sets per muscle group per week. That is achievable across two to three sessions, but it demands more total volume than a pure strength MED approach.
How do I know if my dose is too low?
If your strength numbers on key lifts are not improving over four weeks and your sessions feel consistently easy, your dose is below your adaptation threshold. Add one set per exercise and reassess over the following month.


